Welcome by Luisa Cabal (UNAIDS) Moderator: Susana Fried (CREA and Global Health Justice Partnership) With: Ricki Kgositau (AIDS Accountability International), Oriana López Uribe (BALANCE / RESURJ), Nthabiseng Mokoena (ARASA), Niluka Perera (Youth Voices Count), Jaime Todd-Gher (Amnesty International), Kay Thi Win (Asia Pacific Network of Sex Workers)
Livestream: Beyond Blame – Challenging HIV Criminalisation: Plenary 2 (HJN, 2018)
Welcome to BEYOND BLAME – Challenging HIV Criminalisation, live from De Balie in Amsterdam, 23 July 2018.
11:20 – 12:10 What About Human Rights? The Benefits and Pitfalls of Using Science in Our Advocacy to End HIV Criminalisation Facilitator: Laurel Sprague (UNAIDS) With: Chris Beyrer (John Hopkins Bloomberg School of Public Health), Edwin Cameron (Constitutional Court of South Africa), Richard Elliott (Canadian HIV/AIDS Legal Network), Lynette Mabote (ARASA), Paula Munderi (IAPAC)
12:10 – 13:00 Women and HIV Criminalisation: Feminist Perspectives Facilitator: Naina Khanna (Positive Women’s Network – USA) With: Sarai Chisala-Tempelhoff (Women’s Lawyers Association, Malawi), Michaela Clayton (ARASA), Kristin Dunn (AIDS Saskatoon), Deon Haywood (Women With A Vision)
France: HIV criminalisation laws have a disproportionate impact on women
HIV: The share of women!
For the 8th of March, International Women’s Rights Day, Seronet takes stock of some figures on HIV related to women worldwide.
HIV in the world: women’s numbers
In 2015, globally, about 17.8 million women (aged 15 and over) were living with HIV, equivalent to 51% of the total population living with HIV. About 900,000 of the 1.9 million new HIV infections worldwide in 2015 – 47 percent – were women. It is young women and girls aged 15 to 24 who are particularly affected. Globally, about 2.3 million adolescent girls and young women were living with HIV in 2015, representing 60% of the entire population of young people (aged 15 to 24) living with HIV. 58% of new HIV infections among 15-24 year olds in 2015 were among adolescent girls and young women.
According to the same source, regional differences in new cases of HIV infection among young women and the proportion of women (aged 15 and over) living with HIV compared to men are considerable. They are even more important between young women (aged 15 to 24) and infected young men. In sub-Saharan Africa, 56% of new HIV infections occurred in women, and the rate was even higher among young women aged 15 to 24, accounting for 66% of new infections.
In the Caribbean, women accounted for 35% of newly infected adults, and 46% of new infections occurred among young women aged 15 to 24 years. In Eastern Europe and Central Asia, 31% of new cases of HIV infection have affected women; however, the rate of new infections among young women aged 15 to 24 reached 46%. In the Middle East and North Africa, women represent 38% of newly infected adults, while 48% of young women aged 15 to 24 are newly infected. In Western Europe, Central Europe and North America, 22% of new infections occurred in women, the highest rate among young women aged 15 to 24, with 29% of new infections (1).
Inequalities between women themselves
Some women are more exposed to HIV than others. This is a function of belonging to certain groups. The incidence of HIV in specific groups of women is disproportionate. According to an analysis of studies measuring the cumulative prevalence of HIV in 50 countries, it is estimated that sex workers around the world are about 14 times more likely to be infected with HIV than other women of childbearing age. (2). In addition, data from 30 countries indicate that the cumulative prevalence of HIV among women who inject drugs was 13%, compared to 9% among men who inject drugs (3).
A feminization of the HIV epidemic in France
Over the years, the HIV / AIDS epidemic has been strongly feminized in France too: the share of new diagnoses has increased in France from 13% in 1987 to 33% in 2009. Heterosexual contamination is the main vector of HIV transmission (54% of HIV-positive discoveries) and women make up the majority of these infections. Compared to men, they are infected younger.
In France, women account for about 30% of new HIV infections each year, a significant proportion of whom are born abroad and especially in sub-Saharan Africa. If we look at the 2016 data, we note that among heterosexuals, the majority of diagnostics relates to 2,300 people born abroad. 80% are born in sub-Saharan Africa and 63% are women. Late-stage discoveries are more specific to men than women.
Migrant women, in greater numbers than men in France, suffer more problems related to sexual health: complications specific to pregnancy and childbirth and sexual violence. These states are dependent on the conditions of the country of origin (sexual mutilation, forced marriages), and migration (rape, trafficking in human beings). They can be strengthened upon arrival in the host country, as the period of installation often corresponds to a period of health and social precariousness, which increases the risks of exposure to HIV and sexually transmitted infections.
What factors exacerbate the prevalence of HIV?
It’s obvious … but it’s worth remembering. Violence against women and girls increases their risk of HIV infection (4). A study in South Africa found that the link between intimate partner violence and HIV was more pronounced in the presence of domineering behaviour and high HIV prevalence.
In some settings, up to 45% of adolescent girls report that their first sexual experience was forced. Worldwide, more than 700 million women alive today were married before their eighteenth birthday. Often, they have limited access to prevention information and limited means to protect themselves from HIV infection. Worldwide, out of ten adolescent girls and young women aged 15 to 24, only three of them have complete and accurate knowledge of HIV (5). Lack of information on HIV prevention and the inability to use such information in the context of sexual relations, including in the context of marriage, undermine women’s ability to negotiate condom use and engage in safer sex, says UN Women.
Seropositivity: a double sentence for women
Other data indicate that women living with HIV are at increased risk of violence (6), including violations of their sexual and reproductive rights (reproductive health). Cases of involuntary or forced sterilization and forced abortions among women living with HIV have been reported in at least fourteen countries. In addition, legal standards directly affect the level of risk for women to contract HIV, says the UN Women. In many countries where women are most at risk, the laws that are supposed to protect them are ineffective. The lack of legal rights reinforces women’s subordinate status, particularly with regard to women’s rights to divorce, to possess and inherit property, to enter into contracts, to prosecute and to testify in court, to consent to medical treatment and open a bank account. Discriminatory laws on the criminalization of HIV transmission can also have a disproportionate impact on women, as they are more vulnerable to being tested for HIV and to find out whether or not they are infected with HIV when they access healthcare for their pregnancy. HIV-positive mothers are considered criminals under HIV-related laws in several countries in West and Central Africa, which explicitly or implicitly prohibits them from being pregnant or breastfeeding. for fear that they might transmit the virus to the fetus or to the child (7).
The response to HIV for women
Globally, between 76% and 77% of pregnant women have had access to antiretroviral drugs to prevent mother-to-child transmission of HIV, says UN Women (data for 2015). Despite this encouraging rate, more than half of the 21 priority countries of the UNAIDS Global Plan were unable to meet the need for family planning services for at least 25% of all married women. Another element is that governments are increasingly recognizing the importance of gender equality in HIV interventions at the national level. However, only 57% (out of the 104 countries that submitted data) had a specific budget. For their part, Global Fund expenditures on women and girls have increased from 42 percent of its total portfolio in 2013 to about 60 percent in 2015.
(1): UNAIDS, 2015 estimates from the AIDSinfo online database. Additional disaggregated data correspond to unpublished estimates provided by UNAIDS for 2015, derived from country-specific AIDS epidemic models.
(2) : Stefan Baral and al. (15 mars 2012), “Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis”, The Lancet Infectious Diseases, vol. 12, no 7. p. 542.
(3) : UNAIDS (2014) The Gap Report, p. 175.
(4) : R. Jewkes and al. (2006) « Factors Associated with HIV Sero-Status in Young Rural South African Women: Connections between Intimate Partner Violence and HIV », International Journal of Epidemiology, 35, p. 1461-1468 ;
(5) : UNAIDS (2015) 2015 Report on World AIDS Day “On the Fast-Track to end AIDS by 2030: Focus on Location and Population“, p. 75.
(6) : WHO and UNAIDS (2010) “Addressing violence against women and HIV/AIDS: What works?“, p. 33.
(7) : Commission mondiale sur le VIH et le droit (2012) « Risques, droit et santé », p. 23.
——————————————–
VIH : La part des femmes!
A l’occasion du 8 mars, Journée international des droits des femmes, Seronet fait le point sur quelques chiffres relatifs au VIH concernant les femmes dans le monde.
VIH dans le monde : la part des femmes
En 2015, à l’échelle mondiale, environ 17,8 millions de femmes (âgées de 15 ans et plus) vivaient avec le VIH, soit 51 % de toute la population vivant avec le VIH. Environ 900 000 des 1,9 million des nouveaux cas d’infection par le VIH constatés dans le monde en 2015 – soit 47 % – ont concerné des femmes. Ce sont les jeunes femmes et les adolescentes de 15 à 24 ans qui sont particulièrement touchées. A niveau mondial, environ 2,3 millions d’adolescentes et de jeunes femmes vivaient avec le VIH en 2015, représentant 60 % de toute la population de jeunes (de 15 à 24 ans) vivant avec le VIH. 58 % des nouveaux cas d’infection par le VIH chez les jeunes de 15 à 24 ans en 2015 touchaient des adolescentes et des jeunes femmes.
Selon la même source, les différences régionales concernant les nouveaux cas d’infection par le VIH chez les jeunes femmes et la proportion de femmes (âgées de 15 ans et plus) vivant avec le VIH par rapport aux hommes sont considérables. Elles sont encore plus importantes entre les jeunes femmes (âgées de 15 à 24 ans) et les jeunes hommes infectés. En Afrique subsaharienne, 56 % des nouveaux cas d’infection par le VIH ont touché des femmes, et ce taux a été encore plus élevé chez les jeunes femmes de 15 à 24 ans, représentant 66 % des nouveaux cas d’infection.
Dans les Caraïbes, les femmes ont représenté 35 % des adultes nouvellement infectés, et 46 % des nouveaux cas d’infections ont touché les jeunes femmes de 15 à 24 ans. En Europe de l’Est et en Asie centrale, 31 % des nouveaux cas d’infection par le VIH ont touché des femmes ; toutefois, le taux des nouveaux cas d’infection touchant les jeunes femmes de 15 à 24 ans a atteint 46 %. Au Moyen-Orient et en Afrique du Nord, les femmes représentent 38 % des adultes nouvellement infectés, alors que 48 % des jeunes femmes de 15 à 24 ans sont nouvellement infectées. En Europe occidentale, en Europe centrale et en Amérique du Nord, 22 % des nouveaux cas d’infection ont touché des femmes, ce taux étant plus élevé chez les jeunes femmes de 15 à 24 ans, avec 29 % de nouveaux cas d’infection (1).
Des inégalités entre les femmes elles-mêmes
Certaines femmes sont plus exposées au VIH que d’autres. C’est notamment fonction de l’appartenance à certaines groupes. L’incidence du VIH sur certains groupes spécifiques de femmes est disproportionnée. Selon une analyse d’études mesurant la prévalence cumulée du VIH dans 50 pays, on estime que, dans le monde, les travailleuses du sexe ont environ 14 fois plus de risques d’être infectées par le VIH que les autres femmes en âge de procréer (2). Par ailleurs, d’après des données émanant de 30 pays, la prévalence cumulée du VIH chez les femmes qui consomment des drogues injectables était de 13 %, contre 9 % chez les hommes qui consomment des drogues injectables (3).
Une féminisation de l’épidémie de VIH en France
Au fil des années, l’épidémie à VIH/sida s’est fortement féminisée en France aussi : la part de nouveaux diagnostics est passée, en France, de 13 % en 1987 à 33 % en 2009. La contamination hétérosexuelle est le principal vecteur de transmission du VIH (54 % des découvertes de séropositivité) et les femmes constituent la majorité de ces contaminations. Par rapport aux hommes, elles sont contaminées plus jeunes.
En France, les femmes représentent environ 30 % des nouvelles contaminations par le VIH chaque année, une part importante d’entre elles sont nées à l’étranger et en particulier en Afrique subsaharienne. Si on regarde les données de 2016, on note que les hétérosexuels, la majorité des découvertes de séropositivité est constituée par les 2 300 personnes nées à l’étranger. Il s’agit à 80 % de personnes nées en Afrique subsaharienne et à 63 % de femmes. Les découvertes à un stade avancé concernent plus particulièrement les hommes que les femmes.
Les femmes migrantes, en plus grand nombre que les hommes en France, subissent plus de problèmes liés à la santé sexuelle : complications propres à la grossesse et à l’accouchement, violences sexuelles. Ces états sont dépendants des conditions du pays d’origine (mutilations sexuelles, mariages forcés), et du parcours migratoire (viols, trafic d’êtres humains). Ils peuvent être renforcés à l’arrivée dans le pays d’accueil, la période d’installation correspondant souvent à une période de précarité sanitaire et sociale, qui accroît les risques d’exposition aux VIH et aux infections sexuellement transmissibles.
Quels facteurs exacerbent la prévalence du VIH ?
C’est une évidence… mais qu’il est bon de rappeler. La violence à l’égard des femmes et des filles augmente leurs risques d’infection par le VIH (4). Une étude menée en Afrique du Sud a démontré que le lien entre la violence infligée par un partenaire intime et le VIH était plus marqué en présence d’un comportement dominateur et d’une prévalence élevée du VIH.
Dans certains contextes, jusqu’à 45 % des adolescentes indiquent que leur première expérience sexuelle a été forcée. Dans le monde, plus de 700 millions de femmes en vie aujourd’hui ont été mariées avant leur dix-huitième anniversaire. Souvent, elles disposent d’un accès restreint aux informations de prévention, et de moyens limités pour se protéger contre une infection par le VIH. A l’échelle mondiale, sur dix adolescentes et jeunes femmes de 15 à 24 ans, seulement trois d’entre elles ont des connaissances complètes et exactes sur le VIH (5). Le manque d’informations sur la prévention du VIH et l’impossibilité d’utiliser de telles informations dans le cadre de relations sexuelles, y compris dans le contexte du mariage, compromettent la capacité des femmes à négocier le port d’un préservatif et à s’engager dans des pratiques sexuelles plus sûres, rappelle l’ONU Femmes.
La séropositivité : une double peine pour les femmes
D’autres données indiquent que les femmes vivant avec le VIH sont davantage exposées à des actes de violence (6), y compris des violations de leurs droits sexuels et génésiques (la santé reproductive). Des cas de stérilisation involontaire ou forcée et d’avortements forcés chez les femmes vivant avec le VIH ont été signalés dans au moins quatorze pays. De plus, les normes juridiques affectent directement le niveau de risque pour les femmes de contracter le VIH, rappelle l’Onu Femmes. Dans bon nombre de pays où les femmes y sont le plus exposées, les lois qui sont censées les protéger sont inefficaces. Le manque de droits juridiques renforce le statut de subordination des femmes, en particulier au regard des droits des femmes de divorcer, de posséder et d’hériter de biens, de conclure des contrats, de lancer des poursuites et de témoigner devant un tribunal, de consentir à un traitement médical et d’ouvrir un compte bancaire. Par ailleurs, les lois discriminatoires sur la criminalisation de la transmission du VIH peuvent avoir des répercussions disproportionnées sur les femmes, car elles sont plus exposées à être soumises à des tests de dépistage et ainsi à savoir si elles sont ou non infectées lors de soins au cours de la grossesse. Les mères séropositives sont considérées comme des criminelles en vertu de toutes les lois relatives au VIH en vigueur dans plusieurs pays en Afrique de l’Ouest et en Afrique centrale, ce qui leur interdit, explicitement ou implicitement, d’être enceintes ou d’allaiter, de crainte qu’elles transmettent le virus au fœtus ou à l’enfant (7).
La réponse face au VIH pour les femmes
A l’échelle mondiale, entre 76 et 77 % des femmes enceintes ont eu accès à des médicaments antirétroviraux pour prévenir la transmission du VIH de la mère à l’enfant, indique l’Onu Femmes (données pour 2015). Malgré ce taux encourageant, plus de la moitié des 21 pays prioritaires du Plan mondial d’Onusida ne parvenaient pas à répondre aux besoins en services de planning familial d’au moins 25 % de l’ensemble des femmes mariées. Autre élément : les gouvernements reconnaissent de plus en plus l’importance de l’égalité des sexes dans les interventions face au VIH qui sont menées à l’échelle nationale. Cependant, seulement 57 % (sur les 104 pays qui ont soumis des données) d’entre eux disposaient d’un budget spécifique. De leur côté, les dépenses du Fonds mondial de lutte contre le sida consacrées aux femmes et aux filles ont augmenté, passant de 42 % de son portefeuille total en 2013 à environ 60 % en 2015.
(1) : Onusida, estimations de 2015 provenant de la base de données en ligne AIDSinfo. Les données désagrégées supplémentaires correspondent aux estimations non publiées fournies par l’Onusida pour 2015, obtenues à partir de modèles des épidémies de sida spécifiques aux pays.
(2) : Stefan Baral et al. (15 mars 2012), “Burden of HIV among female sex workers in low-income and middle-income countries: a systematic review and meta-analysis”, The Lancet Infectious Diseases, vol. 12, no 7. p. 542.
(3) : Onusida (2014) The Gap Report, p. 175.
(4) : R. Jewkes et al. (2006) « Factors Associated with HIV Sero-Status in Young Rural South African Women: Connections between Intimate Partner Violence and HIV », International Journal of Epidemiology, 35, p. 1461-1468 ;
(5) : Onusida (2015) Rapport 2015 sur la Journée mondiale de lutte contre le sida “On the Fast-Track to end AIDS by 2030: Focus on Location and Population“, p. 75.
(6) : L’OMS et ONUSIDA (2010) “Addressing violence against women and HIV/AIDS: What works?“, p. 33.
(7) : Commission mondiale sur le VIH et le droit (2012) « Risques, droit et santé », p. 23.
Published in Seronet on March 7, 2018
Ukraine: HIV stigma, threats of violence and a culture of blame make women fearful of disclosing their status or seeking care
Women with HIV abused by partners, rejected by society
Shunned by relatives, doctors and the community, Ukrainian women struggle to survive and protect their children.
Kiev, Ukraine – In October 2012, 31-year-old Hanna Lilina, a Donetsk-native, was told she had HIV during a pre-natal check-up.
When she found out, she felt confused.
“I started to clean my apartment obsessively as if people could contract HIV just by touching a surface. I didn’t understand it, I was so afraid and paranoid,” she says.
Lilina became infected with HIV after having unprotected sex with her boyfriend, whom she suspects contracted the virus by sharing a needle with friends who injected opium.
He had been an abusive partner, and so by the time she discovered she had the virus, they had already parted ways.
“At first, it was just emotional abuse. Then he started to beat me, especially after he had been drinking. It was always worse then,” she says.
Lilina left her partner to rebuild her life in Kiev.
“Telling my family was difficult. My parents were shocked and upset at first but now they’re very supportive. However, my sister immediately assumed that I was a drug addict. She hates me and wants nothing to do with me.”
In Kiev, she started a new relationship.
But when her new boyfriend found out about the virus, “he started acting differently around me”, she says.
“When I was seven months pregnant, he tried to get me to have an abortion. By the time the baby was born, he had left me.”
Ukraine has one of the fastest growing HIV epidemics in Eastern Europe and Central Asia, with approximately 240,000 people living with the virus and a prevalence of 0.9 percent in the general adult population.
In Ukraine, 35 percent of women living with HIV have experienced violence from a partner or husband since the age of 15, compared to 19 percent of women who do not have HIV, according to a November 2016 survey by Positive Women, a Ukrainian NGO.
Approximately half of the 1,000 HIV-positive women surveyed across the country had no support after they suffered violence.
“There is an epidemic of gender-based violence in many regions of the world, disproportionately affecting women and girls, making them more vulnerable to becoming infected with HIV,” Vinay P. Saldanha, UNAIDS regional director for Eastern Europe and Central Asia, tells Al Jazeera.
‘A culture of blame’
According to UN Women, women living with HIV are more likely to experience violence, including violations of their sexual and reproductive rights.
“Involuntary and coerced sterilisation and forced abortion among women living with HIV has been reported in at least 14 countries worldwide,” UN Women reports.
“The relationship between violence and HIV is complicated, but a significant factor is the culture of blame that surrounds HIV.
“In Eastern Europe and Central Asia, as in many other regions, the blame for HIV tends to fall on women,” says Saldanha.
Women are also often the first in a couple to learn of HIV in the family as the coverage of HIV testing and treatment in Ukraine is higher among women.
Most women are tested for HIV at least once at gynaecology and obstetrics clinics.
“It can tragically unfold that her husband or sexual partner points the finger of blame at her, even if her male partner was the one to infect her with HIV.
“In such a situation, she is at potential risk of domestic and sexual violence.”
The consequences can be life-threatening.
“As a result, a woman’s de-facto response can be to refrain from telling her family or partner that she has HIV, and she might even be too afraid to seek out the life-saving health services available,” says Saldanha.
And even if a woman does want treatment, it is not always guaranteed.
In some cases, women are unable to access medical support because their partners refuse to pay for travel to the hospital.
“‘You can get treatment, just not with my money,’ is what they say. But when a woman is financially dependent, what can she do?,” says Sofia, an HIV-positive officer working for the All-Ukrainian Network of People Living with HIV/AIDS, the country’s largest patient organisation.
The situation became so precarious that in May 2017, the Positive Women NGO filed a joint report to the United Nations on the violations of women’s rights, along with other civil society organisations representing drug-users, sex workers and members of the LGBT community.
“In small towns and the provinces, the situation is particularly difficult. It can be impossible for an HIV-positive woman to find a gynaecologist who will voluntarily examine or simply look at her,” says a member of Positive Women, who wished to remain anonymous.
“It’s only on the orders of high authorities that doctors will agree to an examination. And these are cases involving ‘safe’ women.”
If a woman is considered “unsafe” – an alcoholic, drug-user or sex worker – she cannot even enter a doctor’s office.
A community’s attitude to HIV can be so unsupportive that patients are often harassed or forced out.
“Doctor’s attitudes are not much better,” says the Positive Women member.
Sterilisation threats and protecting children
The group’s report to the UN detailed the case of Vera, a sex worker from the Kirovograd region who underwent a caesarean section to deliver her baby.
After the procedure, the 24-year-old was told that she had been sterilised because, in the words of her doctor, she had “no right to build a family and have children”.
“Over a year and a half later, Vera is still coming to terms with what happened to her,” said the Positive Women member.
Mothers are also challenged with having to protect their children from discrimination.
Olga Rudneva, head of the Elena Pinchuk ANTIAIDS Foundation (ANTIAIDS) in Kiev, tells Al Jazeera that mothers often hide their children’s HIV status.
“If, for example, a school director finds out that a student has HIV, the child could be kicked out.
“This leaves some women in extremely poor financial situations, unable to work because they must look after their child. Women prefer to just to pay for a clean medical record to avoid such problems – you can do that in Ukraine,” she says.
Lilina, the HIV patient and domestic abuse survivor, says her daughter’s paediatrician tried to inform her school of the child’s HIV status.
With the help of ANTIAIDS, she managed to block the doctor’s attempt.
“[He] was certainly not happy when he finally agreed to keep my status confidential,” says Lilina.
Government officials failed to respond to Al Jazeera’s repeated requests for comment.
But the Ukrainian government is taking this situation “very seriously”, says UNAIDS’ Saldanha.
In 2017, the National Coordination Council on preventing HIV/AIDS in Ukraine (NCC) accepted two representatives from Positive Women to help create an HIV/AIDS strategy over the next five years.
ANTIAIDS’ Rudneva says there is more to be done, however.
“If you have HIV, you deserve HIV. That’s the mentality in this country,” she says.
The foundation gave Lilina the support to start rebuilding her life in Kiev, helping her helping her find accommodation and providing her baby with a supply of nappies.
It also encouraged her to join Kyyanka, a support group.
At first, Lilina was sceptical and it took her a while to go to a meeting.
“But now the women are like my family,” she says. “It wasn’t until I joined Kyyanka that I understood how I’d been struggling with self-stigma and repressing negative feelings about myself.
“The self-stigma is still there, but at least I’m aware of it now. It’s only when you’re aware of the stigma, that you can start to fight against it.”
Published in Al Jazeera News on February 25, 2018
Africa: Moving towards revolutionising approaches to HIV criminalisation
“We have all agreed with the Sustainable Development Goal of ending HIV and Tuberculosis by 2030. We cannot get there while we are arresting the same people we are supposed to ensure are accessing treatment and living positively,” said Dr Ruth Labode, a member of Parliament from Zimbabwe opening remarks at a two-day global meeting co-hosted by the AIDS and Rights Alliance for Southern Africa (ARASA) and HIV Justice Worldwide (HJWW) on 24 and 25 April 2017 in Johannesburg, South Africa, which focused on “Revolutionising approaches to Criminalisation of HIV Non-disclosure, Exposure and Transmission”.
The meeting was attended by advocates, civil society organisations, lawyers, judges, national human rights institutions and Members of Parliament from all over Africa and with some delegates from North America. Central to these deliberations was the draconian provisions within numerous HIV-specific laws being developed as government responses to the prevention and control of the HIV epidemic. The good intentions inherent in these pieces of legislation are often marred with provisions, which criminalise people based on their HIV status. Punitive provisions relating to ‘compulsory testing’, ‘involuntary partner notification’, ‘non-disclosure’ and ‘transmission’ of HIV are often cited, fueling stigma against people living with HIV.
The common theme binding these deliberations, was the negative impact of HIV criminalisation and the stories that were shared by colleagues. The increasing trend of imposing criminal sanctions against people living with HIV, had resulted in adverse impact on public health outcomes for certain populations, especially women. While reinforcing stigma, HIV criminalisation impedes access to sexual and reproductive health services such as condoms, HIV testing and treatment. Further, HIV criminalisation discourages HIV-positive women from accessing ante-natal care, which leads to increased maternal and child mortality. The overly broad and vague nature of most HIV specific laws, accompanied by the imposition of criminal sanctions without empirical or scientific support, further underpins the rift between public health goals and the protection of human rights.
Representing the AIDS Legal Network, one of the partners who led the development of the 10 Reasons Why Criminalisation Harms Women, Johanna Kehler mentioned the fact that, “HIV criminalisation and HIV specific laws are often set against a social milieu that is patriarchal, heteronormative and perpetuates gender inequalities and utilises punitive approaches to “correct” imbalances.” She went on to add that these laws ultimately maintain and widen the divide between public health needs and human rights obligations.
 “Most prosecutions globally involve no or negligible risk of transmission. Among the thousands of known prosecutions, cases where it was clear, much less proven beyond reasonable doubt, that an individual planned on or wanted to infect another person with HIV, are exceedingly rare. People are being convicted of crimes contrary to the best public health advice, but also contrary to scientific and medical evidence”, said Dr Laurel Sprague of the HIV Justice Network, who has since become the Executive Director of the Global Network of People Living with HIV (GNP+).
“Most prosecutions globally involve no or negligible risk of transmission. Among the thousands of known prosecutions, cases where it was clear, much less proven beyond reasonable doubt, that an individual planned on or wanted to infect another person with HIV, are exceedingly rare. People are being convicted of crimes contrary to the best public health advice, but also contrary to scientific and medical evidence”, said Dr Laurel Sprague of the HIV Justice Network, who has since become the Executive Director of the Global Network of People Living with HIV (GNP+).
During the meeting, various organisations shared their experiences around litigating these matters and community advocacy mounted to reform problematic laws or specific draconian provisions. Cases from Zimbabwe, Nigeria and Niger showcased that challenges were experiences in most contexts.
The Uganda Network on Law, Ethics & HIV/AIDS (UGANET), together with other advocates and activists, continue to challenge the Ugandan law and constitutionality of the criminalisation provisions contained in the HIV Prevention and Control Act of 2014. The Southern Africa Litigation Centre (SALC) spoke to the extensive work that they furthered in Malawi, which included a focus on arbitrary arrests and dentition. Malawi has taken the centre stage where HIV criminalisation is concerned, as they are currently in the process of tabling a decade-old Draft HIV and AIDS (Prevention and Management) Bill, which contains draconian provisions around HIV criminalisation.
Amplifying the voice of survivors of HIV criminalisation, the meeting was privileged to engage with Kerry Thomas via telephone from a state correctional facility in Boise, Idaho in the United States of America. Mr Thomas, who was prosecuted for HIV non-disclosure and the sentence that he is serving, reinforced the unjust nature of these laws. Mr Thomas is currently serving his eighth year out of a 30-year sentence for non- disclosure to his ex-partner, despite there being no proof of transmission and the fact that he had consensual and protected sex. His appeal on the unconstitutionality of Idaho’s non-disclosure law, was overturned in the District courts in 2016.
The meeting concluded with very strong calls for everyone to joining the global HIV JUSTICE WORLDWIDE movement and organisations committed to utilise their existing resources to galvanise advocacy focusing on ending HIV criminalisation.
Participants agreed that there was a need to focus on the inter-sectionalities within the HIV criminalisation discourse, as well as a need for coordination and collaboration amongst legislators, members of the judiciary, parliamentarians, health care workers and civil society organisations to further advocacy related to this issue.
The participants also agreed that transformative approaches to HIV criminalisation, require both legal and social reforms, such as sensitisation of community members and the media. ARASA has committed to working with colleagues in developing a timeline of key events and advocacy opportunities, at which colleagues could participate.
Revolutionising approaches to Criminalisation of HIV Non-disclosure, Exposure and Transmission was supported by a grant from the Robert Carr civil society networks Fund.
Since its inception, ARASA has played an active role in addressing HIV criminalisation in the region and globally. ARASA has strengthened the capacity of civil society on the issue and supported partners to work with the media, parliamentarians, members of the judiciary and lawyers to address HIV criminalisation.
To read more about the meeting, follow #Decrim4Health on Facebook and Twitter. You can also view a gallery of photos taken during the meeting here.
Canada: Alison Carter explores the negative consequences of HIV Criminalisation on women living with HIV
The Politics Of Sex For Women Living With HIV
“If I have sex, I could go to jail.”
This is the reality of life for women living with HIV in Canada.
It’s a story I heard a few weeks ago from an African woman who had recently immigrated to Vancouver and is now faced with the profoundly isolating experience of being a Black HIV-positive woman in Canadian society.
This may come as a surprise to anyone unfamiliar with HIV in Canada: Women (and men) who are living with HIV are at risk of facing a criminal charge of aggravated sexual assault for not disclosing their HIV status before engaging in consensual sex, unless they have a low HIV viral load and use a condom. Beyond serving jail time, those convicted must register as a sex offender, a title usually reserved for child molesters and rapists. “That follows you around forever,” says a woman who was herself imprisoned for HIV non-disclosure.
This woman, and many others, bravely spoke out about their experiences of being treated like a criminal for living with HIV at the annual Canadian Conference on HIV/AIDS Research, held in Montréal from April 6 to 9.
The conference included a special session on the criminalization of HIV non-disclosure, which covered a broad array of issues ranging from data on the total number of charges laid, to women’s personal testimonies of feeling ‘under surveillance’, to the latest research findings on how the law is understood and experienced by thousands of women living with HIV across Canada.
Saara Greene of McMaster University, Angela Kaida of Simon Fraser University, and Marvelous Muchenje of the Canadian Coalition to Reform HIV Criminalization co-hosted the event in partnership with HIV-positive women, which brought together dozens of community leaders, scientists, lawyers, and activists from around the country.
“Some women are suffering in silence and they don’t know what the law says,” said Muchenje.
“The law assumes that sex takes place between partners of equal power,” added Greene. “And it wholly ignores what causes women not to disclose their status, including widespread stigma and violence that are both systematically targeted at women living with this disease.”
The women who have participated in their research, which involved telling stories through participatory arts-based Body Mapping, say “disclosure is not always safe or positive for women’s health and safety.” And for many, the fear of being abused, rejected, or worse jailed, is a significant barrier to even thinking about the idea of getting involved with someone.
Eighteen women have been charged for HIV non-disclosure in Canada, many of whom come from marginalized backgrounds and are survivors of sexual violence.
“Beyond the number of prosecutions, however, is the threat of prosecution,” said Kaida. “And this threat compromises both women’s interactions with healthcare providers and their sexual health.”
Kaida analyzed survey data collected from over 1000 women living with HIV in Canada, and found that for most women (65 per cent), the law affects the amount and type of information they are willing to share with providers, particularly as it relates to their sexual lives.
Kaida also found that 51 per cent of women were not having sex and of these, 78 per cent were intentionally abstinent. Women’s reasons for intentional abstinence were diverse though many (33 per cent) worried about HIV criminalization and disclosing their status to sexual partners.
“Laws criminalizing HIV non-disclosure have been defended as a means of protecting the sexual well-being of women,” Kaida said. “However, our findings show women are protecting themselves from the law by intentionally abstaining from sex.”
It goes without saying that women living with HIV shouldn’t have to live in fear of having sex. Sex is a normal part of life. It feels good. It has health benefits. And it’s a human right, one that this law violates.
The law also ignores groundbreaking new science that shows a person with HIV who is on treatment with undetectable levels of the virus in their blood has zero chance of passing HIV to their sexual partners. Put simply, Undetectable=Untransmittable.
Wedged in between science, on the one hand, and society on the other, are decades of cultural discourses of risk, danger, and stigma.
Stigma is a dangerous construct. It deters people from accessing testing and treatment. It leads to anxiety, depression, isolation, and loneliness. And it creates a social and legal environment that fosters abuse, harassment, and discrimination against women living with the condition.
In the face of a mountain of evidence of medical advances and human rights violations, many people are calling (shouting, really) for policy markers in Canada to update the laws and de-criminalize HIV. Doing so would also help to de-stigmatize sex for women living with HIV.
“The discrimination I face because of I live with HIV is ridiculous,” says Peggy Frank, an openly positive woman and researcher. “It’s a small virus that has little to do with who we are. I am a human being and I have the rights that every other human being has, and that includes sex.”
Allison Carter is a feminist epidemiologist conducting sex-positive research with women living with HIV. She is working with women on building a new online resource, called Life and Love with HIV, dedicated to building conversation and community around sexuality and relationships for women and couples with HIV around the world. Sign up to be notified when the website launches.
Published on April 10, 2017 in the Huffington Post
Mexico: Roberto Guzman on why HIV criminalisation laws do not protect women from HIV or violence and are inappropriate
Women and HIV criminalisation(Google translation – For the original Spanish version, please scroll down)
By Roberto Guzmán
Despite the fact that HIV infection has no cure, it has now become treatable and mortality has fallen. HIV has become a chronic disease with a higher quality of life and life expectancy. However, social perceptions have not significantly changed and HIV transmission and its gender-implications are still the cause of associated stigma and strong discrimination throughout the infection process and have become a major obstacle for prevention and medical care.
If a woman lives with HIV, her discrimination inhibits personalization of the risks for fear of distrust or of criticisms in her social environment, a situation that reduces the possibility of negotiating preventive measures and undermines her willingness towards her partners, by limiting a systemic diagnosis, by not wanting to share her results and her new life condition and by increasing the probability of not being able to seek treatment for its control.
Although the infection rates in this sector remains stable, women who contract HIV today continue to be ostracized, not only by their own families but also by their communities. They are expelled from their homes or rejected by their spouses to live in terror or to suffer violence, even to be deprived of life as if they were criminals.
If our Congress intended to apply a criminal law to the exposure and transmission of HIV as an outlet for this, perhaps its decree resulted from a well-intentioned desire to protect them in response to a legitimate concern for its rapid expansion. But continuing to allow society to criminalize them, does not foresee the emergence of new transmissions or reduce their vulnerability to the virus, on the contrary it would hurt them rather than help them, by having a negative impact on public health needs and the protection to their human rights. Continuing to criminalize them also does not protect them from sexual violence and rape, nor from unwanted pregnancies, on the contrary, it increases the risk of “secondary criminalization” when rape survivors infected with HIV could be persecuted for a possible exposure and transmission to their babies or their partners.
I believe that instead of responding to HIV by raising fears or laws, a human rights approach would emphasize protecting the dignity of all of them by creating conditions for free and informed taking of their health and life.
————————————————-
EL CIELO DE LA OPOSICIÓN
Por Roberto Guzmán
La mujer y su criminalización por VIH
Pese a que la infección del VIH no tiene cura, hoy se vuelve tratable y disminuye su mortalidad al tornarse crónica y con mayor calidad y esperanza de vida. Sin embargo, los cambios en la percepción social que aún continúan son menos significativos ya que su transmisión y sus implicaciones respecto al género son causa de un estigma asociado y motivo de una fuerte discriminación en los distintos ámbitos del proceso de la infección al volverse obstáculo importante para la prevención y su asistencia médica.
Sí una mujer vive con VIH, su discriminación inhibe la personalización que tiene frente al riesgo por miedo a generarse desconfianza o crítica en su entorno social, situación que reduce la posibilidad de que se negocien medidas preventivas y el socavar su predisposición con sus parejas, al limitar su detección sistémica al no querer compartir su resultado y nueva condición de vida y la probabilidad de no poder buscar tratamiento para su control.
Pese a que la tasa de infección de este sector permanece estable, las mujeres que hoy contraen VIH continúan siendo condenadas a un ostracismo, no solo por sus propias familias sino por sus comunidades que las expulsan de sus casas o al ser rechazadas por sus cónyuges teniendo que vivir aterradas o sufrir violencias, incluso ser privadas de la vida como si fuesen criminales.
Si nuestro Congreso tuviera la intención de aplicar una ley criminal a la exposición y transmisión del VIH como una salida a esto, quizá su decreto resultaría un bien intencionado deseo por protegerlas como respuesta a una preocupación legítima por su rápida expansión. Pero el continuar permitiendo que la sociedad las criminalice, no prevé la aparición de nuevas transmisiones ni reduce con ello su vulnerabilidad frente al Virus, al contrario las perjudicaría más que ayudarlas, al lograr un impacto negativo en las necesidades de salud pública y en la protección a sus derechos humanos. El seguir criminalizándolas tampoco las protege de la violencia sexual y la violación, ni de los embarazos no deseados, por el contrario, aumenta el riesgo a una “criminalización secundaria” cuando las sobrevivientes de violación si fuesen infectadas por VIH pudieran verse perseguidas por una posible exposición y transmisión a sus bebes o a sus parejas.
Considero que en lugar de responder al VIH generando temor o leyes, un enfoque de derechos humanos pondría énfasis en la protección a la dignidad de todas ellas al crearse condiciones para la toma libre e informada en relación a su salud y su vida.
Canada: Toronto’s ‘Now’ weekly newspaper prominently features HIV criminalisation impact, advocacy and advocates
This week, Toronto’s weekly newspaper, ‘Now’, features four articles on HIV criminalisation and its impact in Canada.
The lead article, ‘HIV is not a crime’ is written from the point of view of an HIV-negative person who discovers a sexual partner had not disclosed to him. It concludes:
After my experience with non-disclosure, I felt some resentment. But while researching this article, I reached out to the person who didn’t disclose to me. We talked about the assumptions we’d both made about each other. It felt good to talk and air our grievances.
I realized I’d learned something I’d never heard from doctors during any of my dozens of trips to the STI clinic, something I’d never heard from my family, my school, in the media or from the government – that you don’t need to be afraid of people living with HIV.
 A second article, Laws criminalizing HIV are putting vulnerable women at greater risk, highlights the impact HIV criminalisation is having on women in Canada, notably that it is preventing sexual assault survivors living with HIV from coming forward due to a fear they will be prosecuted for HIV non-disclosure (which, ironically, is treated as a more serious sexual assault than rape).
A second article, Laws criminalizing HIV are putting vulnerable women at greater risk, highlights the impact HIV criminalisation is having on women in Canada, notably that it is preventing sexual assault survivors living with HIV from coming forward due to a fear they will be prosecuted for HIV non-disclosure (which, ironically, is treated as a more serious sexual assault than rape).
Moreover, treating HIV-positive women as sex offenders is subverting sexual assault laws designed to protect sexual autonomy and gender equality. Front-line workers and lawyers say they’re hearing from HIV-positive women who are afraid to report rape and domestic abuse for fear of being charged with aggravated sexual assault themselves.
“People come to me all the time who don’t know what to do,” says Cynthia Fromstein, a Toronto-based criminal lawyer who’s worked on 25 to 30 non-disclosure cases. “Canada, unfortunately, is virulent in its zeal to prosecute aggravated sexual assault related to HIV non-disclosure.”
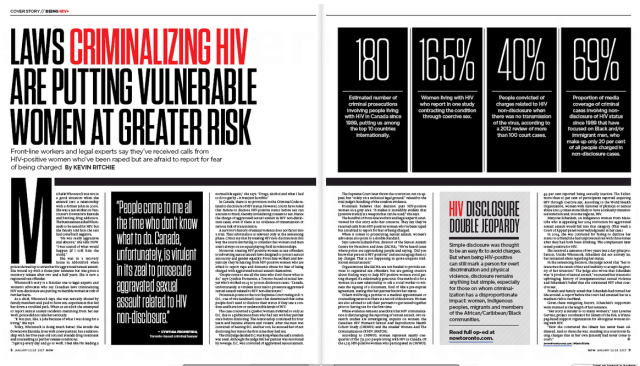 It also features a strong editorial, ‘HIV disclosure double jeopardy’ by the Canadian HIV/AIDS Legal Network’s Cecile Kazatchkine and HALCO’s Executive Director, Ryan Peck, which notes:
It also features a strong editorial, ‘HIV disclosure double jeopardy’ by the Canadian HIV/AIDS Legal Network’s Cecile Kazatchkine and HALCO’s Executive Director, Ryan Peck, which notes:
In a statement that mostly flew under the radar, Minister of Justice Jody Wilson-Raybould declared, on World AIDS Day (December 1), her government’s intention “to examine the criminal justice system’s response to non-disclosure of HIV status,” recognizing that “the over-criminalization of HIV non-disclosure discourages many individuals from being tested and seeking treatment, and further stigmatizes those living with HIV or AIDS.”
Wilson-Raybould also stated that “the [Canadian] criminal justice system must adapt to better reflect the current scientific evidence on the realities of this disease.”
This long-overdue statement was the first from the government of Canada on this issue since 1998, the year the Supreme Court of Canada released its decision on R v. Cuerrier, the first case to reach the high court on the subject.
 Finally, the magazine features a number of promiment HIV activists from Canada, including Alex McClelland, who is studying the impact of HIV criminalisation on people accused and/or convicted in Canada.
Finally, the magazine features a number of promiment HIV activists from Canada, including Alex McClelland, who is studying the impact of HIV criminalisation on people accused and/or convicted in Canada.
US: Discussion about the decriminalisation of HIV takes centre stage at World AIDS day panel in Georgia
A panel of HIV activists and LGBT organizers took aim at laws in Georgia that criminalize people with HIV and can leave them facing prison sentences of up to 20 years.
The discussion about decriminalizing HIV took center stage at a World AIDS Day panel on Nov. 30. People with HIV in Georgia can face a prison term of up to 10 years for having sex with someone without disclosing their HIV status. Even acts like spitting – which do not transmit HIV – are criminalized when directed towards a law enforcement officer with penalties that include up to 20 years of prison time.
Last year, a gay Atlanta man was charged in South Carolina with exposing a sex partner to HIV. Tyler Orr said he did disclose and as the panelists pointed out during the recent discussion, what counts as disclosure and how to avoid “he said, she said” debates in court is unclear.
“What advocates have tried to encourage folks to do in this really unwinnable situation is to have a notarized document or affidavit before you engage in one of these punishable acts,” Mel Medalle of SisterLove told the crowd of about 40 people.
“Which almost never happens, but that is how extreme and absurd this situation is,” Medalle added.
Nina Martinez, a member of the Coalition to End HIV Criminalization in Georgia, pointed out that disclosure laws can also create safety risks for people with HIV.
“Every single time, especially as a woman, every single time, it’s me risking my personal safety,” Martinez said.
Marxavian Jones, who serves as one of Georgia Equality’s Youth HIV Policy Advisors, echoed agreed with Martinez.
“Who is going to defend me when I disclose my status to someone and they take it to social media and decide they want to tell everybody,” Jones said.
The Center for HIV Law & Policy has pointed to the increased risk of intimate partner violence that can come with disclosure, writing that disclosure can “provide an additional excuse, or cover, for physical violence.”
The ongoing stigma of HIV-positive individuals also means that – as Jones pointed out – a disgruntled lover posting a partner’s HIV status to social media can have real consequences, including job loss or being outed to family.
During the National HIV Prevention Conference in Atlanta last year, public health experts and HIV activists argued that rather than criminalizing HIV-positive people, and adding to the stigma they face, people with HIV should be pushed to treatment options.
At the recent panel, participants also highlighted legislation being drafted by the Coalition to End HIV Criminalization in Georgia. The coalition is currently reaching out to legislators to find a sponsor for the bill.
“[The legislation is] so we can repeal, which would completely get rid of it,” Medalle said. “The other option would be to reform it, so to make changes to it but to ultimately have some semblance of it.”
While Medalle said it may seem like a “no brainer that we wouldn’t want this [law],” stigma and other means of criminalizing HIV-positive individuals makes the issue more complicated. In Texas and a handful of other states, there are no specific statutes that target people with HIV but they are still prosecuted under other laws including reckless endangerment.
Reforming the law means that advocates can create better standards for prosecutions, and can “craft a law that comports with modern HIV science, what we know about the routes of transmission,” Medalle said.
Martinez, who is a member of the coalition, said the HIV criminalization law in Georgia also falls short in other aspects.
“The law in Georgia doesn’t require intent to infect, it doesn’t require likelihood of transmission because it has things like spit, urine, feces in it. It doesn’t require transmission,” Martinez said.
The Georgia law also doesn’t take into account issues like condom usage or advising a partner to take PEP (post-exposure prophylaxis) after sexual intercourse – acts which reduce the likelihood of transmission. The reforms to the law would change that, the panelists said.
Emily Halden Brown, a Georgia Equality field organizer who organized the panel discussion, said the event highlighted how people with HIV are impacted by it.
“I think the most valuable moment in all of the discussions I’ve ever been a part of on this, are the moments where people living with HIV share the stories of how they are directly impacted,” Brown said. “Anytime someone shares their personal story you can just feel the change in the audience.”
The event was hosted by Georgia Equality, SisterLove, and The Counter Narrative Project at Gallery 874. The panel discussion coincided with the “Living With” art exhibit, which featured art about the experiences of living with HIV. A closing reception helped raise funds for Georgia Equality’s HIV policy work.
Published in Project Q on Dec 12, 2016
Canada: Canada’s sexual assault laws, as currently applied, put women living with HIV at increased risk of harm
Women living with HIV facing double jeopardy
Canada’s sexual assault laws are being applied in ways that, ironically, put some women at increased risk of harm. Women living with HIV are stuck between a rock and a hard place. If they disclose their HIV status to an intimate partner, they may be exposed to violence. If they don’t, they could go to jail for sexual assault.
People who fail to disclose HIV can be charged with fraud, invalidating sexual consent. They can be prosecuted for aggravated sexual assault, the most serious form of the crime, normally reserved for rapes compounded by physical violence. Conviction carries a penalty up to life in prison, and lifelong registry as a sex offender — even when there is no transmission of HIV nor any meaningful risk.
There is broad scientific consensus that when HIV is managed with anti-retroviral therapies, the risk of transmission is negligible, even without a condom. Today’s treatments can reduce viral loads to undetectable levels. Unfortunately, our courts haven’t caught up with the science. Legal practices are at odds with public health. Rather than hazard jail, people at risk of HIV may seek refuge in ignorance, choosing not to get tested.
Recently, Attorney General and Justice Minister Jody Wilson-Raybould acknowledged: “The criminal justice system must adapt to better reflect the current scientific evidence. . . . This could include a review of existing charging and prosecution practices.”
The statement was welcomed by Cécile Kazatchkine, senior policy analyst with the Canadian HIV/AIDS Legal Network and a member of the Ontario Working Group on Criminal Law and HIV Exposure. The organization has been working since 2009 to engage provincial attorneys general in developing prosecutorial guidelines that would limit prosecution to cases of intentional transmission. Foot-dragging on change has exposed Canada to increasing international criticism.
Kazatchkine believes the International AIDS Conference in Durban this past July may have been a turning point in the evolving federal position. During a plenary session Justice Edwin Cameron, South Africa’s first openly gay and HIV-positive Constitutional Court judge, singled out two nations with terrible records on HIV criminalization. “He mentioned Zimbabwe and he mentioned Canada,” she notes.
This message was compounded in the recent report by the UN Committee on the Elimination of All Forms of Discrimination Against Women, which called attention to Canada’s “harsh criminal sanctions” for nondisclosure. The report joins a chorus of international organizations recommending criminalization be limited to intentional transmission of the virus.
Criminalizing nondisclosure has had a particularly harsh impact on women, who often fear admitting they are HIV-positive will provoke violent reactions. Of some 180 prosecutions to date, Kazatchkine says, at least 18 of the defendants are women, many of whom were already marginalized by poverty or abuse.
Some of the women contracted the virus while being sexually assaulted themselves; now they’re being labelled sex offenders. The law’s application also has a disproportionate impact on Aboriginal women, who comprise at least six of 18 known female defendants.
Kazatchkine sees progress toward meaningful dialogue: Minister Wilson-Raybould’s statement “is having an impact.” At a roundtable Monday with several provincial ministries, participants got a keen sense of how women with HIV are caught between prosecution and potential violence. Kazatchkine was encouraged when Tracy MacCharles, the minister responsible for women’s issues, suggested the issue could be brought before the Ontario Roundtable on Violence Against Women.
The government has not committed to specific action. But advocates are cautiously optimistic that things are finally moving in the right direction.
Published in St. Catharines Standard on Dec 10, 2016