The HIV Justice Network is a proud supporter of the Support. Don’t Punish campaign now in its ninth year. Tomorrow, Saturday 26 June, is the campaign’s yearly high point, the Global Day of Action.
According to the campaign’s website, “Support.Don’t Punish is a global grassroots-centred initiative in support of harm reduction and drug policies that prioritise public health and human rights. The campaign seeks to put harm reduction on the political agenda by strengthening the mobilisation capacity of communities targeted by the “war on drugs” and their allies, opening dialogue with policy makers, and raising awareness among the media and the public.”
The theme for this year’s Global Day of Action is “Undoing the ‘war’, building the future that our communities have always deserved”. The date, 26th June is symbolic as it is used by most governments to commemorate the International Day Against Drug Abuse and Illicit Trafficking to highlight their so-called ‘achievements’ in “the war on drugs.”
TheSupport. Don’t Punish campaign aligns with the following key messages:
The drug control system is broken and in need of reform.
People who use drugs should no longer be criminalised.
People involved in the drug trade should not face harsh or disproportionate punishments, where retained.
The death penalty should never be imposed for drug offences.
Drug policy should focus on health, well-being, and harm reduction.
Drug policy budgets need rebalancing to ensure health and harm reduction-based responses are adequately financed.
Last year, despite the COVID-19 pandemic, the Global Day of Action saw 288 events in 239 participating cities in 90 countries. The activities organised were incredibly varied and involved over 150 community representatives. In twelve of the regions, networks of people who use drugs were joined by initiatives from convergent movements (including people living with HIV, sex workers, and service providers), strengthening a solidarity block against criminalisation.
This year, we urge you to join the Support.Don’t Punish Global Day of Action. Visit their homepage to check out where activities are taking place near you, and use these resources to amplify the campaign’s messages on social media, including on Facebook, Twitter and Instagram.
HJN commemorates the International Day Against Homophobia, Transphobia and Biphobia!
Today, May 17, is celebrated globally as the International Day Against Homophobia, Transphobia, and Biphobia (IDAHOT).
According to the May 17 website, the day “represents a major global annual landmark to draw the attention of decision-makers, the media, the public, corporations, opinion leaders, local authorities, etc. to the alarming situation faced by people with diverse sexual orientations, gender identities or expressions, and sex characteristics.”
This is a day to not only say no to violence and discrimination against LGBT+ persons but also a rallying cry to ensure equality, dignity, and full respect for human rights of all sexual and gender minorities, including all LGBT+ living with HIV.
The day was created in 2004 to draw attention to the violence and discrimination experienced by LGBT+ people and all other people with diverse sexual orientations, gender identities or expressions, and sex characteristics. The date of May 17 was specifically chosen to commemorate the World Health Organization’s decision in 1990 to declassify homosexuality as a mental disorder.
The theme for this year is “Together: Resisting, Supporting and Healing”
At HJN, we note that HIV still disproportionately affects many in theLGBT+community. In many regions of the world, punitive laws and practices against LGBT+ individuals continue to block effective responses to HIV. Evidence and experience have shown that punitive laws and practices drive sexual minorities away from HIV services.
Some of these punitive practices include criminalisation of same-sex relationships, ‘effeminate’ behavior, cross-dressing, sodomy, and ‘gender impersonation.’
To learn more, this Wednesday, the UK’s All-Party Parliamentary Groups on HIV & AIDS; Global LGBT+ Rights; and STOPAIDS will host a virtual parliamentary event: HIV and the criminalisation of LGBT+ communities to mark the International Day Against Homophobia, Transphobia, and Biphobia.
The event will bring together leading HIV and LGBT+ community representatives from around the world. Through a panel discussion and Q&A, they’ll be exploring the barriers that LGBT+ communities face from realising their right to health and how parliamentarians and the UK Government can advance the decriminalisation of LGBT+ and HIV.
Chaired by Rt Hon David Mundell MP, panelists include:
Joel Simpson – Managing Director, Guyana’s Society Against Sexual Orientation Discrimination (SASOD Guyana)
Simran Shaikh, Co-Founder of Rajmala Welfare Society and Director Transgender Health at John Hopkins University School of medicine
It’s Valentine’s Month! February is historically the month of love, and a time to show and share the love.
The HIV Justice Network is pleased to support campaigns in the month of love – February – focusing on HIV-positive living, loving, and justice.
Given the difficulty that some people living with HIV can face when it comes to finding love, including negotiating disclosure, sex for pleasure, and/or creating a family in the context of HIV criminalisation, it is important to acknowledge that everyone is deserving of love and affirmation.
To this end, the HIV Justice Network wishes to acknowledge the following Valentine’s campaigns for and about people living with HIV.
The #LovePositiveWomen campaign is a global initiative running every Feb 1st-14th for each of us to express, share and support women living with HIV or as a friend of the community. It was developed and led by the International Community of Women Living with HIV (ICW), one of seven founding partners of HIV JUSTICE WORLDWIDE.
The campaign uses social media to link local grassroots gestures of love to each other. Using Valentines Day as a backdrop, #LovePositiveWomen “creates a platform for individuals and communities to engage in public and private acts of love and caring for women living with HIV.”
Going beyond romantic love to deep community love and social justice, the campaign is also a call to action. The HIV Justice Network has been supporting this campaign since 2017.
“#LovePositiveWomen is a response to the lack of attention and support and to make commitments. It requires participants to spend time reflecting on how they as either a woman living with HIV or an ally will commit to loving women living with HIV. Through action, change can be made to fueling economies of love and compassion. Working from a place of strength, it focuses on the idea of interconnectedness, relationship building, loving oneself, and loving one’s community. By starting from a place of love, within oneself, there are endless ways that the negative impacts that HIV has on women living with HIV can be lessened.”
#LoveandAccountability Campaign – What are you loving?
Initiated by Accountability International, their annual Valentine’s campaign has focused on a variety of thematic areas including consent, Resolution 275, and challenging criminalisation, among others.
For this year, their focus will feature some key messages around love, advocacy, human rights, justice, and accountability.
“Accountability International is well known for our fun and innovative Valentine’s Day campaigns and our collaborative, diverse, and inclusive way of working, so this year we have decided to put our Valentine’s campaign on steroids.”
Watch out for HJN’s Executive Director to be a part of the campaign, which uses the hashtags #LoveandAccountability and #LoveandHumanRights.
With love,
The HJN Team
The Importance of Human Kindness and Connection: Sero’s Holiday Card Project
In an era where the term ‘lockdown’ is used to limit our movements, spare a thought for the many prisoners living with HIV (some of whom have been unjustly convicted under HIV criminalisation laws) who are experiencing real lockdowns and severe isolation.
With community support interventions becoming increasingly formalised, and NGOs pushed to operate in terms of strategic plans, deliverables, outputs and outcomes, Sero’s Holiday Card Project stands as a rare example of an organisation recognising the worth of a project focused solely on gestures of basic human kindness.
Last year, the project delivered Holiday cards to around 900 incarcerated people, most of whom are living with HIV. For some, it was the only mail they received all year.
So how did the Holiday Card Project come to be, has it made a difference, and how can you help this year?
Back in the 1980s and ’90s, Cindy Stine lost a lot of friends to HIV. In 1996, just before effective treatments became available, she lost a close friend who was like a son. She made a promise to him that she would continue to be involved in the AIDS response. That’s a promise she’s kept.
Cindy Stine of the Sero Project
In 2011, Cindy was serving on the board of a local LGBT centre when she invited two speakers from the fledgling Sero Project to speak at an event. The speakers were Sean Strub, Sero’s Executive Director, and Robert Suttle. Sean introduced the audience to the concept of HIV criminalisation, a new issue for most, including Cindy. Robert talked about what it means to live as an HIV criminalisation survivor, explaining that as the result of an HIV non-disclosure charge, he served six months in the Louisiana state prison and would be registered as a sex offender for 15 years. Robert showed an image of his driver’s license, with ‘sex offender’ stamped in bold red lettering: ID he has to show often and in many different circumstances.
Cindy approached Sean and Robert to let them know that she wanted to help. A few days later, Sean rang Cindy and invited her to his office where he showed her a stack of letters that Sero had received from people in prison. Sean asked Cindy if she’d volunteer to take on the task of answering the letters. She agreed.
Things could have ended there, with Cindy answering people’s individual letters, but as Cindy read those letters week after week, each letter more heart-breaking than the last, she began to really appreciate the isolation, loneliness and desperate need for connection experienced by many of those inside. She talked it over with her Sero colleagues, and they decided their efforts to build a movement against HIV criminalisation needed to expand to be more inclusive of those who were incarcerated; those directly impacted by HIV criminalisation. They decided to explore how they could support development of a prisoners’ network, starting by compiling a database of contact details of those who’d written.
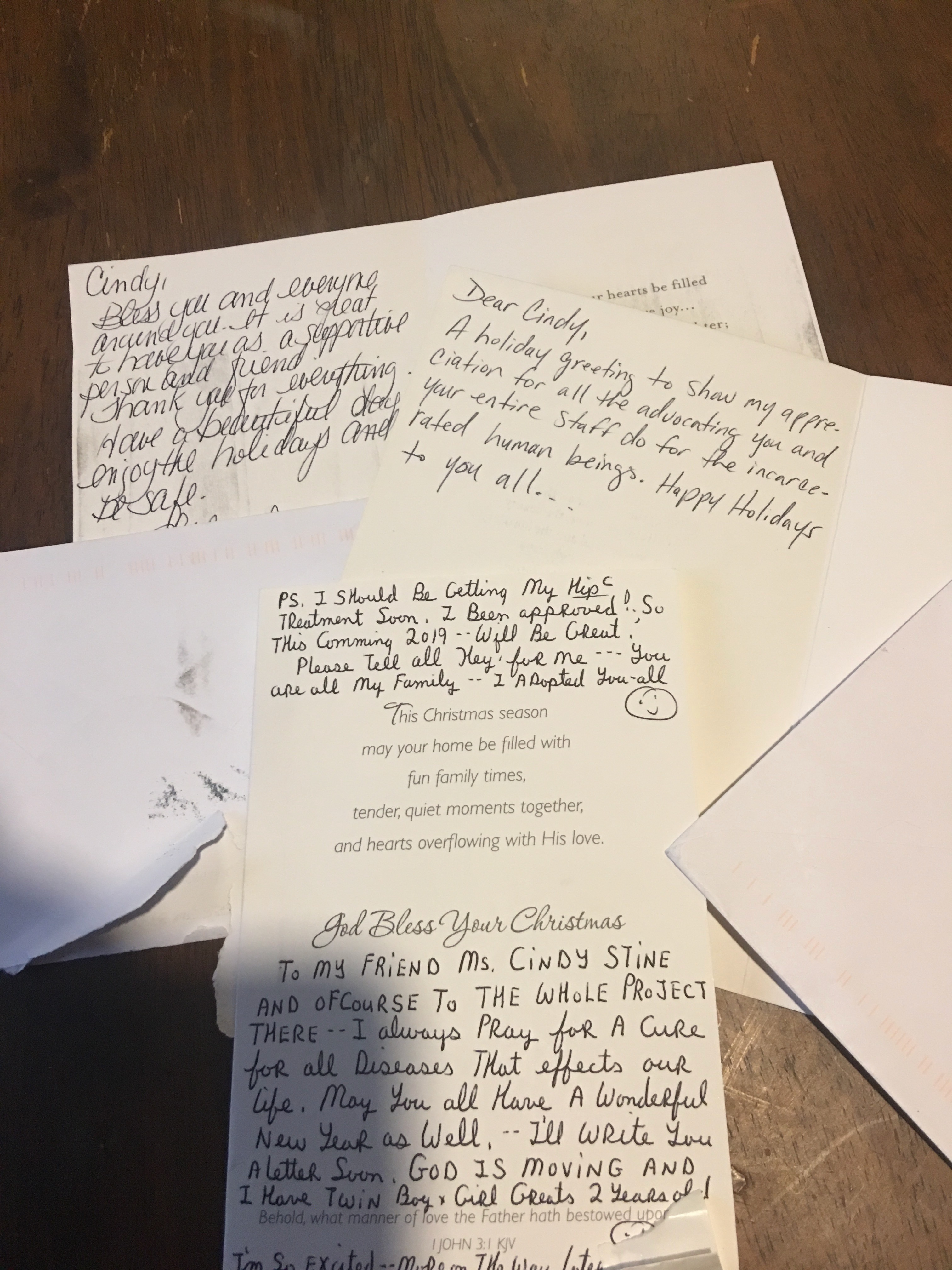
As Sero grew, Cindy was employed to take on community education and other projects but her work answering prisoners’ letters continued. Cindy says of those letters, “sometimes the people writing didn’t even have access to paper, so they’d write on any scrap of paper they could find – recycled envelopes or bits of paper torn off something else. Many of those sending letters weren’t really literate but they wanted to communicate.”
As the 2015 Holiday season approached, Cindy found the letters got harder to read. “A lot of people wrote about loneliness and about their families disowning them after finding out they had HIV, or were gay, or were transgender. People felt they’d been thrown away and forgotten.” Then she had a simple thought, “Wouldn’t it be nice for them to know that they’re not alone.” Then another, “We should send Holiday cards”. She took the idea to Sean, who agreed.
By then, Cindy’s database was so large that she realised Sero would need to prioritise who got cards, focusing on those who were incarcerated as a result of HIV, or they had HIV or another debilitating illness. Cindy also wanted to ensure each person got at least three or four cards but … how to go about it? Cindy put out a call to the 900 or so people on the Sero list-serve asking if anyone was interested in writing some Holiday cards. The response was overwhelming. Many offered to help, with some asking to do 20 cards, some asking to do 200.
The Holiday Card Project has continued each year since then. People express an interest, Cindy sends them a list of first names; they write message on the cards, put them in blank envelopes and return them to Sero; Cindy sorts them, addresses them, and mails them off.
Those who write cards come from all different parts of the community, including some working in other HIV advocacy organisations, some parents of prisoners, and some people living with HIV. People are asked not to ask personal questions but to write messages of support: things like ‘hope you’re doing well’, ‘we’re thinking of you’, and ‘you’re not forgotten’. Some write about themselves, their experience living with HIV, their thoughts and prayers. Some write, ‘we’re thinking of you when we fight HIV criminalisation’.
Sero’s staff and volunteers
One group gets together and spends a day each year writing Holiday cards. People come from all over, saying it feels really good coming into a non-judgemental space and writing messages from the heart. Sometimes Sero will set up a table at a conference and invite people to write cards. Others write cards at home. People feel involved. Each step in the process has meaning: the choice of card, the choice of words, with many people sending their cards with stamps to send them on, to further support the project.
Last Holiday season, about 900 people received cards in facilities across the US, including people on death row. The responses from those who received cards is humbling. Some said, it was the only card they’d received all year, but those cards meant that they knew they were not forgotten. They couldn’t describe the feeling of hearing someone from the mailroom say, ‘You’ve got mail’. They knew that somebody out there had thought enough of them to send a card. Recently Cindy received a letter from a man who’s recently been released. He said that for the last three years he’d so looked forward to those cards as it was the only mail he got. It meant a lot that people had taken the time to write.
The project is not without its challenges. Cindy spends considerable time keeping track of people, as prisoners are often moved. There are also major issues regarding mail screening. Although Cindy has worked to build a rapport with those managing mail distribution at many of the prisons, that hasn’t guaranteed mail is always received. Mail screening rules differ from state to state, institution to institution, and the rules keep changing. Some prisons have now banned cards altogether, some won’t allow glue or glitter or coloured paper, etc. If mail is considered contraband it may be thrown out or returned to Sero. That process has at times driven Cindy to photocopy returned cards, sending the copies in the hope the person will still receive the good wishes.
The Holiday Card Project may have modest goals – to show compassion and care to those who feel abandoned, but it has delivered far more. It has made a difference to the lives of many, letting them know that there are people outside of prison ready to provide support. It has raised awareness about HIV criminalisation and provided a mechanism for people to show they care. It has also helped build trust between prisoners and Sero, a facor that has proven critical to the development of a stronger prisoners’ network and greater engagement with Sero. A stronger prisoners’ network has meant more support for those inside, and it has also resulted in other great projects, like Turn It Up, the health magazine that includes information about HIV for those in prison, largely written by people who are, or have been, incarcerated.
Some of Sero’s Holiday cards
While Sero is best known for its HIV criminalisation reform programmes, its efforts to support network building and empowerment have proven equally important. Sero operates from the belief that those most directly impacted should be at the centre of this work, which is why facilitating the creation and strengthening of networks of People Living with HIV and allies, particularly those representing key populations, remains critical and a priority.
Every year the Holiday Card Project has grown, with prisoners writing to Cindy to let her know if they’ve been moved to another facility. Others write saying, “a friend of mine got cards. Can I be put on the list?” Parents get in touch too, asking for their children to be added to the list, and also writing letters of thanks for cards received.
Still, Cindy thinks there is room for the project to grow; sending cards for holidays celebrated by other religions at other times of the year, and also considering whether cards could be sent for some non-religious events, such as Halloween or Thanksgiving. That way the project can become more inclusive and people won’t have to wait an entire year for mail. Of course, that will mean attracting more people to write cards so that more people can receive them.
If you’re interested in supporting the work of the Holiday Card Project, please contact Cindy at cindy.stine@seroproject.com, Subject – Holiday Card Project.
US: New initiative to combat Anti-Black racism, end criminalisation of pandemics and abolish systems of imprisonment
As Calls for Justice Echo Around the United States, National Groups Led by Most-Policed Communities Affected by HIV and COVID-19 Join in Partnership
The Health Not Prisons Collective Vows to Combat Anti-Black Racism, End Criminalization of Pandemics and Abolish Systems of Imprisonment
June 18, 2020: The Health Not Prisons Collective is a new, three year national initiative of longtime collaborators led by, and accountable to, communities most affected by HIV criminalization in the United States: Counter Narrative Project, Positive Women’s Network – USA (PWN), Sero Project, Transgender Law Center, and the U.S. Caucus of People Living with HIV (The Caucus).
HIV criminalization is the wrongful use of a person’s HIV-positive status in a criminal prosecution, including charging people living with HIV (PLHIV) under HIV-specific criminal statutes, or under general criminal statutes, for behaviors which would not be crimes if the person did not have HIV. There is little legal or other support available for those charged with HIV crimes, yet the consequences of being charged under an HIV criminalization law are severe, even without conviction, and persist long after a person leaves the criminal justice system.
Collectively, and with steadfast allies, the founders of the Collective have pushed criminalization to the forefront of the HIV policy agenda. Now, in the first year of the COVID-19 pandemic, the Collective will build the power of the intersectional national HIV movement led by Black, Indigenous and people of color (BIPOC), women, LGB people, and transgender and gender non-conforming people (TGNC) to refocus our efforts instead of blame, punishment and the denial of basic needs.
Criminalization is never a solution to health challenges. Communities that are already heavily surveilled, policed, and criminalized bear the brunt of HIV criminalization are at the highest risk of harm from COVID-19 related surveillance, policing, criminal charges and/or penalty enhancements. A response rooted in policing and criminalization not only undermines public health and human rights, but jeopardizes the long-term survival of our communities.
“The specifics of the COVID-19 pandemic may be unprecedented — but the racial disparities, intensification of stigma and marginalization, and threats of criminalization in the COVID-19 pandemic are sadly not unanticipated to those of us living with HIV,” said Andrew Spieldenner of the U.S. Caucus of People Living with HIV. “As we work together to overturn the criminalization of HIV baked into policies and laws decades ago, we will also urge our communities and leaders to repudiate the panic and reactive thinking that says police, prosecutors and prisons are the way to handle public health emergencies like COVID-19.”
With support from Gilead Sciences, the Collective’s three-year strategy incorporates political education and training; grassroots and grasstops organizing; policy analysis and advocacy; legal intervention; and narrative change designed to shift discourses about HIV, risk, blame, responsibility, and the role of the carceral state in public health, centering racial and gender justice.
“Most HIV criminalization laws in the U.S. were established at a time when less was understood about HIV transmission. There’s no evidence it has ever contributed to HIV transmission reduction. Today, it directly contradicts current public health efforts to encourage people to know their HIV status and engage in health care and treatment; very few laws have been updated in light of advances in scientific advancements,” explained Tami Haught of Sero Project.
“We can’t stop HIV or COVID-19 criminalization without recognizing the underlying politics of racism, blame and bias that fuel them,” said Charles Stephens of Counter Narrative Project “Only a strategic and sustained movement led by those most targeted by criminalization ourselves and that changes the very narratives of blame in our society will overcome the root conditions that make it politically feasible to pin harm on vulnerable individuals from targeted communities.”
“Successful advocacy to end HIV criminalization requires centering PLHIV and those from overpoliced communities. Despite limited resources, members of the Collective have already had significant success in advancing the community and public discourse as well as influencing policy,” explained Cecilia Chung of Transgender Law Project. “We must now remove the remaining barriers that stop our leaders, including transgender and gender non-conforming Black and brown people, disabled people and others, from scaling up our movement and winning the freedom to thrive as we are.”
Due to lack of resources, work on HIV criminalization to date has largely been episodic, resulting in less coordination and varying results. This coordinated, strategic, multi-year effort will fill a critical gap at the nexus of policy, grassroots organizing, movement building, increasing political will to decriminalize, and culture change at a vital time. The Collective urges funders and people of privilege to invest in multi-year initiatives, honoring the passion and truths of communities with the resources it takes to rapidly scale efforts to win significant, lasting change.
“Our members are on the frontlines of pandemics, and they’re also deep in the resistance to overturn the system that profits from anti-Black racism and violence,” said Naina Khanna of Positive Women’s Network – USA. “We need to honor their commitment and vision with resources. Ongoing dedicated funded initiatives have the best chance to shift the social, legal and political landscape of our nation.”
If you need help with a pandemic-related prosecution or threat, contact Sero Project for HIV-related issues and Community Resource Hub for COVID-19-related issues.
The Foundation partners with Gilead Sciences, Inc. and the Health Not Prisons Collective on a major, multi-state effort to decriminalize HIV and modernize laws that lead to the discrimination of people living with HIV.
LOS ANGELES, June 18, 2020 /PRNewswire/ — The Elizabeth Taylor AIDS Foundation (ETAF) announced today a new national initiative focused on the modernization of criminal laws and penalties for people living with HIV. The effort will launch in partnership with Gilead Sciences, Inc., and a national alliance of advocacy partners including The Counter Narrative Project, Positive Women’s Network, The Sero Project, Transgender Law Center, and the US People Living with HIV Caucus. The Artemis Agency, a Los Angeles-based social impact firm, will be working with ETAF on the public education and awareness campaign. ETAF will also partner with state-based organizations as needed to ensure the initiative’s success.
Catherine Brown, ETAF Executive Director explains, “Very simply, science and the law have not caught up with each other on this issue, there is a disparity between what science tells us and what the laws and statutes in more than 30 states believe. HIV is not a crime, and those living with HIV are being held back by harmful laws and policies that discourage people from getting tested and treated.”
Gilead Sciences, Inc., a research-based biopharmaceutical company with headquarters in Foster City, California, is committed to the initiative and to supporting ETAF and The Health Not Prisons Collective.
“Gilead is proud to support this critical work against the criminalization of HIV,” said Brett Pletcher, Executive Vice President of Corporate Affairs and General Counsel. “These outdated and unjust laws disproportionately affect marginalized communities and further perpetuate the misinformation and stigma that result in decreased testing and poorer health outcomes. This collaborative initiative creates the possibility for systemic change that moves us closer to our collective vision of a more just society, free from discrimination and othering.”
On June 25th, ETAF will host a virtual town hall event to launch the initiative and address the effects of the current environment on the HIV community, as racial inequality and COVID-19 have disproportionately affected and threatened the lives of those who have been incarcerated as a result of their HIV status.
The campaign to modernize criminal laws and penalties that target people living with HIV will focus its initial efforts in Nevada and Ohio, where staffers will work with local advocates to prepare and introduce legislation. The effort also intends to address issues of insurance discrimination against people living with HIV in California, and will support legislation introduced in Missouri once COVID-19 restrictions are lifted for lawmakers in that state.
About The Elizabeth Taylor AIDS Foundation Working tirelessly on the AIDS crisis through the 1980s, Elizabeth Taylor established The Elizabeth Taylor AIDS Foundation (ETAF) in 1991 to reach her vision of an AIDS-free world. ETAF works to provide the direct care needed for people living with and affected by HIV and AIDS. Emphasizing Elizabeth’s commitment to marginalized communities, ETAF’s work ensures that HIV prevention education and access to treatment are available through domestic and international initiatives. HIV Decriminalization nationally, is ETAF’s primary advocacy initiative. We now have the necessary tools to stop the spread of HIV and end the AIDS crisis with sufficient resources.
Media Contacts Catherine A. Brown Executive Director cbrown@etaf.org 310-339-3643
SOURCE The Elizabeth Taylor AIDS Foundation
HIV JUSTICE WORLDWIDE Steering Committee Statement on COVID-19 Criminalisation
Measures that are respectful of human rights and the empowering of communities are more effective than punishment and imprisonment.
As the world struggles with a new global pandemic, law- and policymakers are taking drastic measures in an attempt to minimise the spread of SARS-CoV-2, the virus that causes COVID-19. The situation continues to evolve rapidly and, as it does so, our liberties are being limited in unprecedented ways.
We remind law- and policymakers that each and every limitation of rights should satisfy the five criteria of the Siracusa Principles, as well as be of a limited duration and subject to review and appeal. These principles are:
The restriction is provided for and carried out in accordance with the law;
The restriction is in the interest of a legitimate objective of general interest;
The restriction is strictly necessary in a democratic society to achieve the objective;
There are no less intrusive and restrictive means available to reach the same objective;
The restriction is based on scientific evidence and not drafted or imposed arbitrarily, that is in an unreasonable or otherwise discriminatory manner.
We also warn law- and policymakers against the temptation to use the criminal law or other unjustified and disproportionate repressive measures in relation to COVID-19. These measures can be expected to have a devastating impact on the most vulnerable in society, including those who are homeless and/or living in poverty, as well as individuals from marginalised and already stigmatised or criminalised communities – especially where no economic and social support is provided to allow people to protect themselves and others, including through self-isolation.
Criminalisation disproportionately impacts the most marginalised, stigmatised and the already criminalised people and communities in society.
Criminalisation is not an evidence-based response to public health issues. In fact, the use of the criminal law most often undermines public health by creating barriers to prevention, testing, care, and treatment – for example, people may not disclose their status or access treatment for fear of being criminalised. It can also lead to ill-informed ‘trial’ by social and news media, and to a myriad of human rights violations, from arbitrary arrests and detentions to unfair trials (or no trials at all under new emergency measures) and harsh prison sentences. This can also lead to the spread of infections and communicable diseases in prisons and is of particular relevance in the context of COVID-19, which reveals, once again, the need to address overcrowding and other poor healthcare and sanitation conditions that are all too common in prisons and other closed settings.
Our experience has taught us that hastily drafted laws, as well as law enforcement, driven by fear and panic, are unlikely to be guided by the best available scientific and medical evidence – especially where such science is unclear, complex and evolving. Given the context of a virus that can easily be transmitted by casual contact and where proof of actual exposure or transmission is not possible, we believe that the criminal justice system is unlikely to uphold principles of legal and judicial fairness, including the key criminal law principles of legality, foreseeability, intent, causality, proportionality and proof.
The human rights of those involved in criminal cases related to COVID-19 are at risk of being ignored or violated.
We therefore urge law- and policymakers, the media, and communities at large, to keep human rights front and centre as we collectively respond to a new public health crisis in a climate of fear and uncertainty. It is more critical than ever to commit to, and respect, human rights principles; ground public health measures in scientific evidence; and establish partnerships, trust, and co-operation between law- and policymakers and communities.
“While we recognize the severity of the current health crisis and acknowledge that the use of emergency powers is allowed by international law in response to significant threats, we urgently remind States that any emergency responses to the coronavirus must be proportionate, necessary and non-discriminatory,” the experts said. “Restrictions should be narrowly tailored and should be the least intrusive means to protect public health.” Also, authorities must seek to return life to normal and must avoid excessive use of emergency powers to indefinitely regulate day-to-day life.”
UNAIDS also issued guidance last week that included a number of recommendations, including recommending that States “avoid the use of criminal laws when encouraging behaviours to slow the spread of the epidemic”, noting that empowering and enabling people and communities to protect themselves and others will have a greater overall effect.
And, as described in a recent open letter by more than 800 public health and legal experts in the United States providing recommendations to government officials: “Voluntary self-isolation measures [combined with education, widespread screening, and universal access to treatment] are more likely to induce cooperation and protect public trust than coercive measures and are more likely to prevent attempts to avoid contact with the healthcare system.”
Human rights are key to ending the epidemics
OPINION: End epidemics by breaking down human rights barriers to health
Access to healthcare is a right, not a luxury. We have an historic opportunity to rid the world of HIV, TB and malaria. Let’s seize that opportunity.
Peter Sands is the executive director of The Global Fund to Fight AIDS, Tuberculosis and Malaria and Antonio Zappulla is the chief executive of the Thomson Reuters Foundation.
Among the many challenges involved in improving health services, one is both pervasive and largely hidden. Human rights-related barriers to health, some explicit, others expressed in behaviours and norms, prevent millions of people from access to lifesaving prevention and treatment.
Think of a girl who is forced to get married at 15 and needs her husband’s permission to undergo an HIV test, or to get a bed net to protect herself and her children from malaria. Or a gay man who is beaten up by police and charged with sodomy when he secretly visits the home of a community health care worker to obtain condoms. Or a group of miners working 14 hours a day deep in a mine without ventilation and health insurance despite widespread tuberculosis.
Money alone cannot ensure and protect basic human rights for people most at risk from infectious diseases.
If the media stokes the appetite for a witch hunt against LGBT+ people or condones violence against women, how will society behave? If laws allow abuse and discrimination to be justified, how can social justice be achieved?
Stigma, ignorance, prejudice and lack of opportunities are some of the toughest road blocks to remove. But the combined power of the law and the media can make a difference.
Fair and balanced news coverage is critical in informing public opinion. Respect for human rights is essential to ensure access to health services. Combined, they become the key to unlocking systemic change.
In sub-Saharan Africa, women and girls are twice as likely to be HIV-positive compared to young men. Contributing factors include gender inequality, violence and limited access to education. Meanwhile, men who have sex with men, people who inject drugs, sex workers and transgender people often lack access to health programmes. The root cause? Social taboos, punitive laws and fear of arrest.
Framing health as a human right creates an obligation on states to ensure accessible, acceptable and affordable health care of appropriate quality. But this conception of health as a human right is not shared around the world. You have only to look, for example, at how HIV non-disclosure, exposure and transmission is still criminalized in 86 jurisdictions worldwide.
We will never end the epidemics of HIV, TB and malaria – which killed 3 million people in 2017 alone – unless we dismantle social and human rights barriers to health services.
Everyone has a right to healthcare, encompassing dignity and respect. Not only is this a basic human right, but it is critical to fostering social stability and boosting economic growth. It is predicted that drug-resistant TB will cost the global economy approximately US$17 trillion by 2050 if progress is not made fast enough.
The Global Fund and the Thomson Reuters Foundation are joining forces to combine the power of an international health financing organization with global media and legal expertise, to help break down barriers to health services.
Each year, the Global Fund mobilizes and invests more than US$4 billion to support health programs run by local experts in more than 100 countries. Through its “Breaking Down Barriers” Initiative, the Global Fund is working with countries to reduce human rights-related barriers to health services: to ensure that everybody, including the most marginalized, also have access to prevention, treatment and care services; to see that health care workers are trained not to discriminate against, turn away, or fear people living with HIV or TB; to ensure that police are sensitized to support LGBT people to access prevention and treatment, rather than subject them to extortion, arbitrary arrest and violence; and to inform women, girls and others most affected by disease and violence about their rights and access to legal support. In the last three years, over US$120 million have gone to these and other programs to reduce stigma and discrimination and increase access to justice, an unprecedented investment in human rights as a critical component of our efforts to end HIV, TB, and malaria.
But more needs to be done. In its new partnership with the Global Fund, the Thomson Reuters Foundation will facilitate legal services and support for civil society partners in key countries, including development of “know your rights” training, capacity-building for health practitioners, services providers and their clients, plus guidance for NGOs and civil society groups working in challenging social contexts. The Thomson Reuters Foundation will also train journalists on human rights and health issues, and support awareness-raising on human rights-related barriers to health. Our hope is that by combining forces, we can achieve real impact.
Access to healthcare is a right, not a luxury. We have an historic opportunity to rid the world of HIV, TB and malaria. Let’s seize that opportunity.
On Human Rights Day, please endorse the EECA Statement against HIV Criminalization
Today, December 10, 2019, Human Rights Day, National and Regional Networks and Civil Society Organizations on HIV Criminalization in the EECA Region are asking you to support the movement against HIV criminalization by endorsing the following Statement.
On November 25-26, 2019, the “Decriminalization of HIV transmission in the EECA region: the role of civil society and advocacy tools” meeting was held in Minsk, Belarus, by the Eurasian Women’s Network on AIDS (EWNA), the Global Network of People Living with HIV (GNP+) and CO “100 PERCENT LIFE”. Activists representing national, regional and international networks discussed the current situation with HIV criminalization in the EECA region and options available to strengthen the movement in order to counter that HIV criminalization in the EECA region.
HIV criminalization is a global issue that undermines human rights and impedes the development of public health and, as a result, weakens the efforts to eradicate the HIV epidemic. An analysis of recent HIV criminalization cases shows that they do not reflect the demographics of local epidemics, and the likelihood of persecution is compounded by discrimination against marginalized groups on the basic of drug use, ethnicity, gender identity, immigration status, sex work and sexuality.
The Global Commission on HIV and the Law, the United Nations Development Program (UNDP) and the Joint United Nations Program on AIDS (UNAIDS), among others, declare that any use of criminal law against people living with HIV should be strictly limited to exceptional cases of intentional and malicious HIV transmission to another person and only where real harm occurred. However, the law and law enforcement practice go beyond this limitation in many countries.
According to HIV Justice Worldwide, Europe and Central Asia is the region with the second highest number of laws criminalizing HIV exposure, non-disclosure and transmission. 18 of the 19 countries where such laws have been adopted are in the EECA region. Many of them allow criminal prosecution for actions that do not pose a risk of HIV or pose a low risk only. These laws do not recognize condom use or low viral load as a means of protection against prosecution. They criminalize oral sex, individual breastfeeding cases, as well as bites, scratches, bites, or spitting. Such laws were developed in the times when efficient ARV therapy was not yet available and the HIV diagnosis was equated with a death sentence. The implementation of such laws is most often informed by myths, misconceptions on HIV transmission ways, and stigma against people living with HIV and vulnerable communities.
The laws of the EECA countries criminalizing the HIV transmission vary in their severity and in specific sanctions. The Russian Federation and Belarus are global and regional leaders in terms of the number of criminal cases related to HIV6. In Uzbekistan, a person living with HIV can be prosecuted regardless of whether his/her partner wants to initiate a criminal case. In 2019, a punishment was introduced in the law in Tajikistan for those who refuse to receive HIV therapy7. In many EECA countries, the punishment for any crime involving an HIV-positive person is exacerbated by the positive HIV status.
Concerned by the fact that prosecutions are not always informed by the best available scientific and medical evidence, 20 of the world’s leading HIV scientists have presented the Expert consensus statement on the science of HIV in the context of criminal law.
The criminalization of HIV transmission is a growing human rights issue in Eastern Europe and Central Asia. This fact is also confirmed by the first regional report, prepared in 2017 using the data of the communities of women living with HIV. The study was organized and conducted by EWNA with the support of GNP+ and HIV Justice Worldwide.
The study has shown that HIV criminalization is a gender issue10. The stories and cases documented in the report and other recently conducted studies illustrate that women are more likely to be persecuted, as they are often the first to become aware of their status through regular HIV testing during pregnancy, but they are less likely to safely disclose their HIV positive status to their partner due to gender inequality in the family, economic dependence and high levels of violence. In addition, women living with HIV are less likely to receive adequate legal assistance and to have competent representation in court. In their stories, women talk about violence, threats, and blackmail associated with their HIV-positive status. The laws adopted were designed to protect women from HIV. Unfortunately, this is not the case in the reality as HIV criminalization makes women more vulnerable to violence and structural disparities. HIV criminalization increases the vulnerability of women to deprivation of parental rights, property loss, and poverty.
EECA activists make essential efforts to advocate for the decriminalization of HIV infection. Thus, the active advocacy work conducted by the community of people living with HIV pushed Belarus to adopt an important legislative amendment: the HIV-positive partner should be exempt from criminal liability if he or she has timely warned the HIV-negative partner about HIV and the latter has voluntarily agreed to take actions, which created a risk of infection. However this step alone is not sufficient to solve the issue of HIV criminalization.
We call attention of the EECA countries to the fact that in a society with low stigma and discrimination, people are more likely to be voluntarily tested for HIV and, learning about their status, begin ARV treatment.
We urge communities of people living with HIV and other criminalized and marginalized communities, in particular sex workers, LGBT people, people who use drugs, to unite and take a consolidated position to counter HIV criminalization, presenting a united front against HIV stigma and discrimination embedded in the law.
We urge governments and parliamentarians to use general law to prevent HIV transmission in the harm to health context and, instead of applying criminal law in any cases other than actual infection transmission by malicious intent, take steps to encourage people to be tested, take ARV treatment, communicate their HIV status and have safe sex without fear of stigma, discrimination and violence. This can be achieved by adopting and applying anti-discrimination laws and organizing public information campaigns to dispel myths about HIV, as such campaigns are evidence-based and are led by people living with HIV.
We urge prosecution agencies and prosecutors, to use scientific evidence and evidence-based medicine, in particular the evidence included in the Expert consensus statement on the science of HIV in the context of criminal law, in pre-trial and trial proceedings, in order to limit or prevent abuse of criminal prosecution in cases of allegations of HIV transmission or exposure or in cases of non-disclosure of HIV status.
We urge the media to stop demonizing people living with HIV, presenting us as criminals and as sources of infection. We request the media to consider HIV related issues from the perspective of human rights and use facts and evidence-based medicine while covering such issues.
We encourage donors to invest in communities and advocates opposing HIV criminalization, which undermines human rights and public health.
US: Growing number of Ohio public health experts and advocates call for reform of HIV criminalisation law
Experts: Ohio law on HIV status disclosure hurts public health
COLUMBUS, Ohio — A growing number of Ohio public health experts and advocates are now working to stop what they call the criminalization of HIV.
Daphne Kackloudis, Chief Public Policy Officer at Equitas Health, told News 5 Ohio’s current law charging someone who fails to disclose their HIV status with a felony in all cases is hurting public health.
Kackloudis said the threat of up to eight years in prison is causing too many people to avoid getting tested, because according the current law if someone doesn’t get tested, and isn’t aware of their status they can’t be prosecuted.
“It is a disincentive for someone to get tested, and that’s not good for an individuals health and the public health,” Kackloudis said.
“We want them to get on antiretroviral therapy to get as healthy as possible, and be virally suppressed so they can not transmit HIV.”
Kackloudis believes the potential penalty should be moved back to a misdemeanor in cases where those charged are on HIV medication and are a far less infection risk.
She said the current law allows someone to file charges against an HIV-positive partner, even if they didn’t get the virus from that partner.
She also made it clear she fully understands why the law was created, and said the proposed change in the law would still allow for full prosecution of those who willingly give others HIV.
Graig Cote of Columbus, who has been HIV positive for 33 years, told News 5 changes in the law are needed because it’s too difficult to prove if someone made proper disclosure of their status or not, unless there was a witness or if it was in writing or recorded.
“If we don’t change the laws, people don’t get tested, if they don’t get tested they don’t know if they’re HIV positive,” Cote said.
“We’re not asking for a free ride, we’re just asking that the laws catch up with the science.”
Cote said he hopes the proposed change in Ohio law is ready to present at the statehouse in the first quarter of 2020, and again made it clear the effort would not keep those who willingly spread HIV from facing full prosecution.
“People who want to infect somebody need to be stopped, there’s no dispute about that,” Cote said.
You can select your preferred language from the 'Select Language' menu at the top of the page.
Continue
We use cookies to ensure that we give you the best experience on our website. By continuing to use our site, you are agreeing to our use of cookies. You can change your cookie settings at any time if you want. Find out more in our Privacy & Cookie Policy.